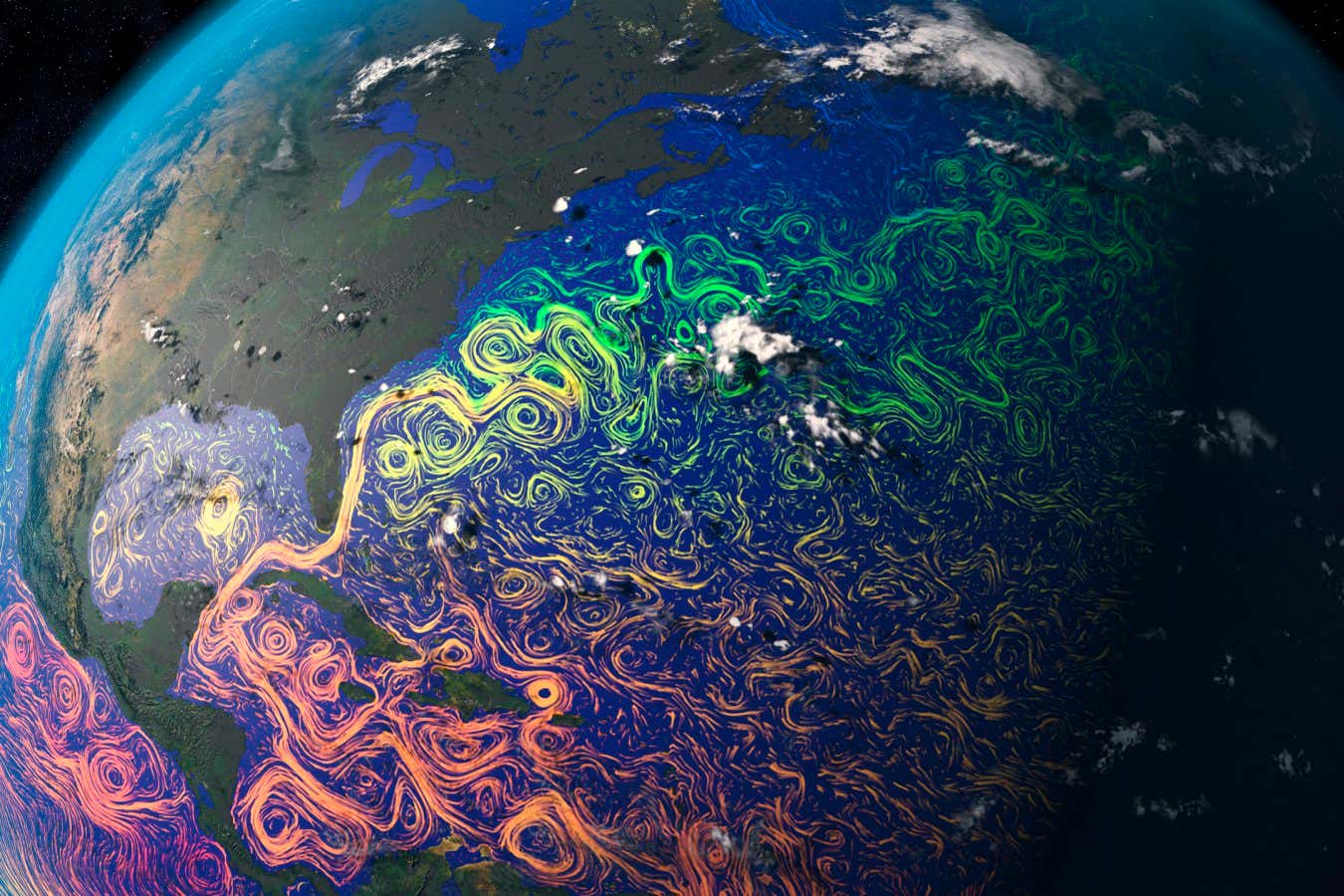
Scientists worry that a surge of meltwater from Greenland could irreversibly collapse the Atlantic Meridional Overturning Circulation, but new modelling suggests the weakening of the current could be reversed if CO2 levels come back down
Simple rules. Infinite complexity. Physicist Stephen Wolfram has spent forty years working out the connection. Here’s the short version.
❍ Subscribe to The Well on YouTube: https://bit.ly/welcometothewell.
❍ Up next: Why the answers to big questions are fundamentally unknowable | L.A. Paul • Why the answers to big decisions are funda…
Physicist Stephen Wolfram spent decades running computer experiments on simple rules — not looking for anything grand, just seeing what happened. What he found turned into a model of how the universe works, an explanation for why evolution never gets stuck, and a mathematical argument for why your life can’t be shortcut or predicted by anyone.
Read the full video transcript: https://bigthink.com/videos/the-unive…
❍ About The Well ❍
Do we inhabit a multiverse? Do we have free will? What is love? Is evolution directional? There are no simple answers to life’s biggest questions, and that’s why they’re the questions occupying the world’s brightest minds.
Support this channel on Patreon to help me make this a full time job: / whatdamath (Unreleased videos, extra footage, DMs, no ads)
Alternatively, PayPal donations can be sent here: http://paypal.me/whatdamath.
Get a Wonderful Person Tee: https://teespring.com/stores/whatdamath.
More cool designs are on Amazon: https://amzn.to/3QFIrFX
Hello and welcome! My name is Anton and in this video, we will talk about the new explanation for what time actually is and a creation of a mini universe in the lab.
Links:
https://journals.aps.org/prresearch/p…
#time #physics #boseeinsteincondensate.
0:00 Experiment that changes how we think about time.
1:30 Measuring the mini universe.
2:05 What is Bose-Einstein Condensate?
3:00 Entropy?
3:50 The problem of time.
5:08 How this was tested.
6:05 Mini Big Bang and the simulation of time.
7:05 Results and what this means for the idea of time.
8:00 Strange observations.
9:05 Implications and conclusions.
Enjoy and please subscribe.
Bitcoin/Ethereum to spare? Donate them here to help this channel grow!
bc1qnkl3nk0zt7w0xzrgur9pnkcduj7a3xxllcn7d4
or ETH: 0x60f088B10b03115405d313f964BeA93eF0Bd3DbF
The hardware used to record these videos:
Abstract:
Alzheimer’s disease (AD) is a prevalent neurodegenerative disorder characterized by β-amyloid (Aβ) deposition, tau protein hyperphosphorylation, and synaptic dysfunction. In recent years, 40 Hz sensory stimulation—including visual, auditory, and multimodal modalities—has emerged as a novel, non-invasive intervention demonstrating potential efficacy in both animal models and preliminary clinical studies. Preclinical evidence indicates that such stimulation can markedly reduce cerebral Aβ burden (by approximately 37%–53%), inhibit tau protein phosphorylation, enhance neuronal network synchrony and synaptic plasticity, and improve learning and memory performance. Limited human trials suggest that 40 Hz sensory stimulation is safe and well tolerated in patients with mild cognitive impairment (MCI) and early-stage AD, with a slowing trend in cognitive scale score decline following intervention. This review summarizes the mechanisms of action, experimental evidence from animal models, and advances in clinical application of 40 Hz sensory stimulation in AD prevention and treatment. It further explores the potential for multimodal combination therapies integrating sensory stimulation with cognitive training, pharmacological interventions, and lifestyle modifications, and addresses challenges such as optimal timing of intervention and the influence of ambient electromagnetic fields in real-world settings. Current evidence supports 40 Hz sensory stimulation as a feasible, multi-target, and safe adjunctive intervention; however, its efficacy and applicability must be verified through multicenter, randomized controlled trials with long-term follow-up.

Confidential Computing (CC) safeguards data during processing, not just storage or transmission. It allows sensitive data, such as cryptographic keys, AI agent reasoning stages, and proprietary algorithms, to be computed safely without external access or modification. As AI systems become more independent and interconnected, confidential computing ensures computation integrity and privacy end-to-end.
PROMOTED.
Neuromorphic computing has the potential to overcome limitations of traditional silicon technology in machine learning tasks. Recent advancements in large crossbar arrays and silicon-based asynchronous spiking neural networks have led to promising neuromorphic systems. However, developing compact parallel computing technology for integrating artificial neural networks into traditional hardware remains a challenge. Organic computational materials offer affordable, biocompatible neuromorphic devices with exceptional adjustability and energy-efficient switching. Here, the review investigates the advancements made in the development of organic neuromorphic devices. This review explores resistive switching mechanisms such as interface-regulated filament growth, molecular-electronic dynamics, nanowire-confined filament growth, and vacancy-assisted ion migration, while proposing methodologies to enhance state retention and conductance adjustment. The survey examines the challenges faced in implementing low-power neuromorphic computing, e.g., reducing device size and improving switching time. The review analyses the potential of these materials in adjustable, flexible, and low-power consumption applications, viz. biohybrid spiking circuits interacting with biological systems, systems that respond to specific events, robotics, intelligent agents, neuromorphic computing, neuromorphic bioelectronics, neuroscience, and other applications, and prospects of this technology.
Keywords: Brain-inspired neuromorphic computing; Neuromorphic bioelectronics; Neuroscience; Organic materials; Resistive switching mechanisms.
© 2025. The Author(s).
Over the past decade, the artificial neural networks domain has seen a considerable embracement of deep neural networks among many applications. However, deep neural networks are typically computationally complex and consume high power, hindering their applicability for resource-constrained applications, such as self-driving vehicles, drones, and robotics. Spiking neural networks, often employed to bridge the gap between machine learning and neuroscience fields, are considered a promising solution for resource-constrained applications. Since deploying spiking neural networks on traditional von-Newman architectures requires significant processing time and high power, typically, neuromorphic hardware is created to execute spiking neural networks. The objective of neuromorphic devices is to mimic the distinctive functionalities of the human brain in terms of energy efficiency, computational power, and robust learning. Furthermore, natural language processing, a machine learning technique, has been widely utilized to aid machines in comprehending human language. However, natural language processing techniques cannot also be deployed efficiently on traditional computing platforms. In this research work, we strive to enhance the natural language processing traits/abilities by harnessing and integrating the SNNs traits, as well as deploying the integrated solution on neuromorphic hardware, efficiently and effectively. To facilitate this endeavor, we propose a novel, unique, and efficient sentiment analysis model created using a large-scale SNN model on SpiNNaker neuromorphic hardware that responds to user inputs. SpiNNaker neuromorphic hardware typically can simulate large spiking neural networks in real time and consumes low power. We initially create an artificial neural networks model, and then train the model using an Internet Movie Database (IMDB) dataset. Next, the pre-trained artificial neural networks model is converted into our proposed spiking neural networks model, called a spiking sentiment analysis (SSA) model. Our SSA model using SpiNNaker, called SSA-SpiNNaker, is created in such a way to respond to user inputs with a positive or negative response. Our proposed SSA-SpiNNaker model achieves 100% accuracy and only consumes 3,970 Joules of energy, while processing around 10,000 words and predicting a positive/negative review. Our experimental results and analysis demonstrate that by leveraging the parallel and distributed capabilities of SpiNNaker, our proposed SSA-SpiNNaker model achieves better performance compared to artificial neural networks models. Our investigation into existing works revealed that no similar models exist in the published literature, demonstrating the uniqueness of our proposed model. Our proposed work would offer a synergy between SNNs and NLP within the neuromorphic computing domain, in order to address many challenges in this domain, including computational complexity and power consumption. Our proposed model would not only enhance the capabilities of sentiment analysis but also contribute to the advancement of brain-inspired computing. Our proposed model could be utilized in other resource-constrained and low-power applications, such as robotics, autonomous, and smart systems.
Keywords: SpiNNaker; artificial neural network; natural language processing; neuromorphic computing; sentiment analysis; spiking neural networks.
Neural networks have enabled great advances in recent times due mainly to improved parallel computing capabilities in accordance to Moore’s Law, which allowed reducing the time needed for the parameter learning of complex, multi-layered neural architectures. However, with silicon technology reaching its physical limits, new types of computing paradigms are needed to increase the power efficiency of learning algorithms, especially for dealing with deep spatio-temporal knowledge on embedded applications. With the goal of mimicking the brain’s power efficiency, new hardware architectures such as the SpiNNaker board have been built. Furthermore, recent works have shown that networks using spiking neurons as learning units can match classical neural networks in supervised tasks. In this paper, we show that the implementation of state-of-the-art models on both the MNIST and the event-based NMNIST digit recognition datasets is possible on neuromorphic hardware. We use two approaches, by directly converting a classical neural network to its spiking version and by training a spiking network from scratch. For both cases, software simulations and implementations into a SpiNNaker 103 machine were performed. Numerical results approaching the state of the art on digit recognition are presented, and a new method to decrease the spike rate needed for the task is proposed, which allows a significant reduction of the spikes (up to 34 times for a fully connected architecture) while preserving the accuracy of the system. With this method, we provide new insights on the capabilities offered by networks of spiking neurons to efficiently encode spatio-temporal information.
Keywords: Artificial neural networks; Event processing; MNIST; Neuromorphic hardware; SpiNNaker; Spiking neural networks.
Copyright © 2019 Elsevier Ltd. All rights reserved.