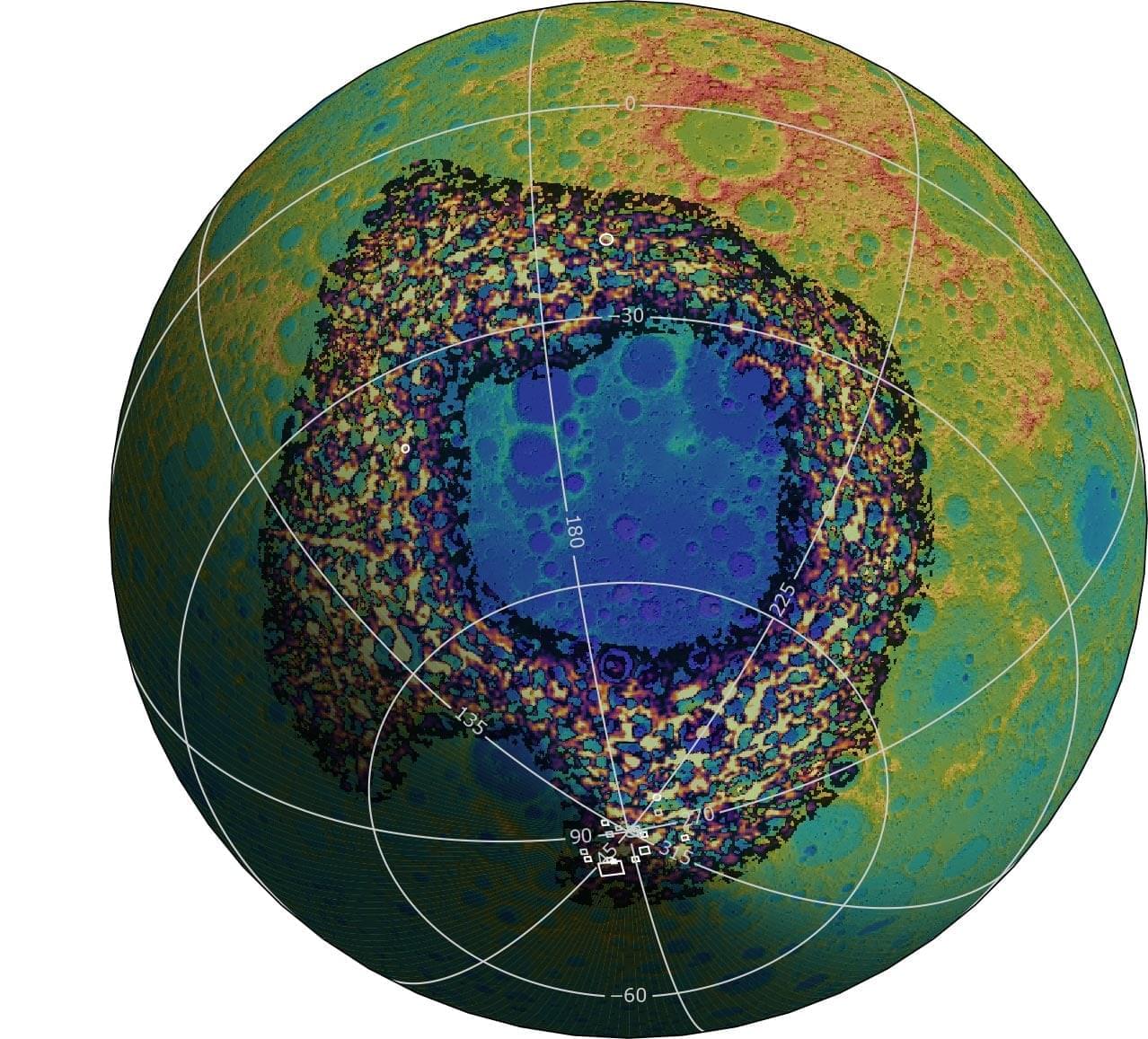
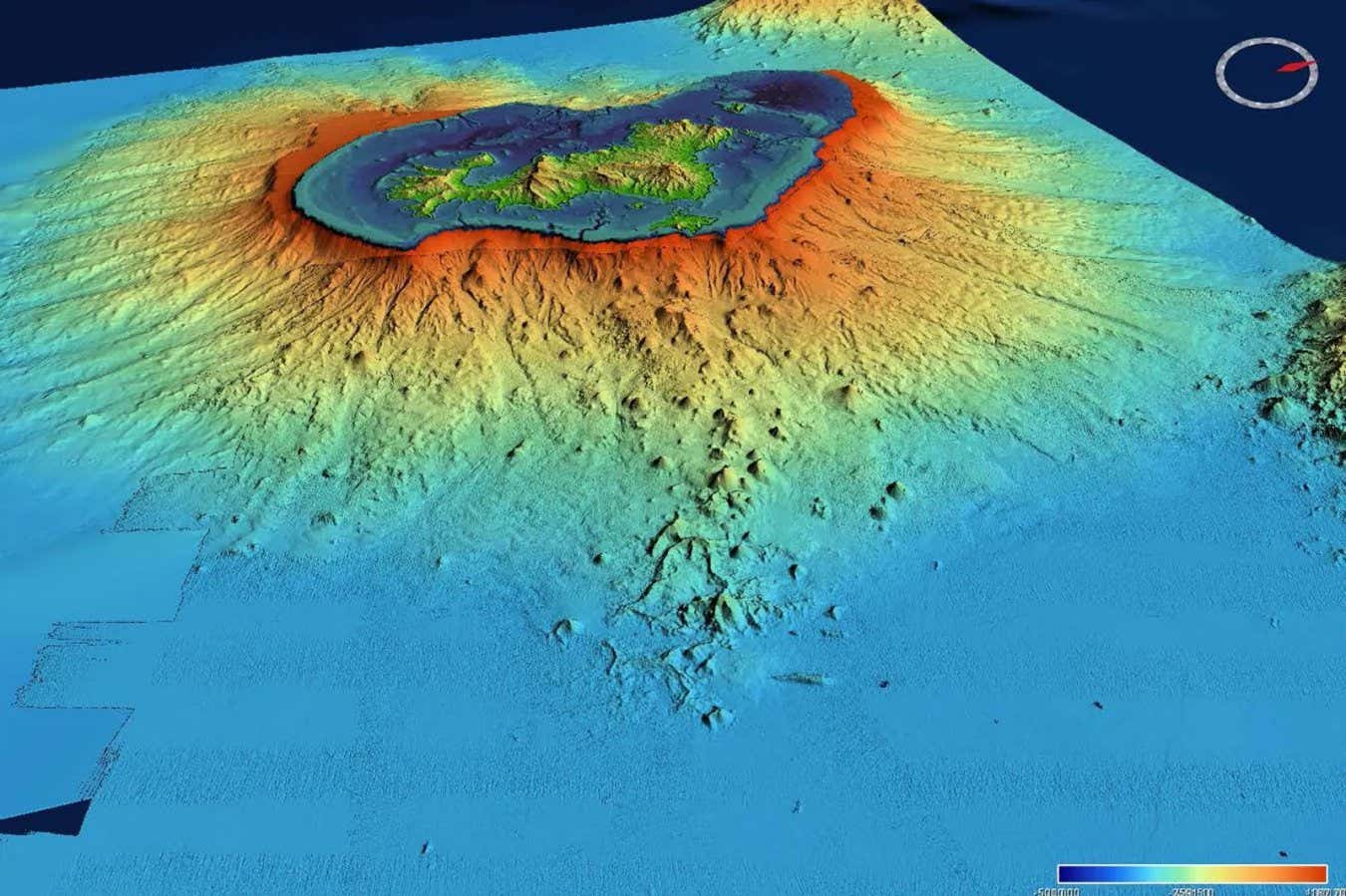
Future Artemis astronauts may be able to explore rocks blasted from deep inside the Moon by an ancient giant impact.

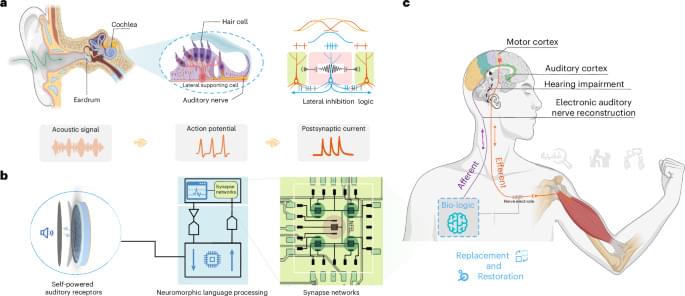
Hearing loss affects millions of people, requiring technology to repair their auditory pathway. A biohybrid interface is developed that combines a self-powered acoustic device and an artificial auditory neural circuit, enabling restoration of auditory function in a rabbit model of hearing impairment.


Cisco confirmed that attackers are now exploiting a Unified Communications Manager (Unified CM) vulnerability patched in early June.
Unified CM (formerly known as Cisco CallManager) is the central control system for Cisco IP telephony systems, handling call routing, device management, and telephony features.
Threat actors without privileges can exploit the vulnerability (CVE-2026–20230) remotely in low-complexity server-side request forgery (SSRF) attacks by sending a crafted HTTP request.